



- Revenue Cycle Management
- COVID-19
- Reimbursement
- Diabetes Awareness Month
- Risk Management
- Patient Retention
- Staffing
- Medical Economics® 100th Anniversary
- Coding and documentation
- Business of Endocrinology
- Telehealth
- Physicians Financial News
- Cybersecurity
- Cardiovascular Clinical Consult
- Locum Tenens, brought to you by LocumLife®
- Weight Management
- Business of Women's Health
- Practice Efficiency
- Finance and Wealth
- EHRs
- Remote Patient Monitoring
- Sponsored Webinars
- Medical Technology
- Billing and collections
- Acute Pain Management
- Exclusive Content
- Value-based Care
- Business of Pediatrics
- Concierge Medicine 2.0 by Castle Connolly Private Health Partners
- Practice Growth
- Concierge Medicine
- Business of Cardiology
- Implementing the Topcon Ocular Telehealth Platform
- Malpractice
- Influenza
- Sexual Health
- Chronic Conditions
- Technology
- Legal and Policy
- Money
- Opinion
- Vaccines
- Practice Management
- Patient Relations
- Careers
UPDATE: Focus on practice #36
Medicare fees; malpractice; Rx ads.
UPDATE
Focus on Practice
By Joan R. Rose
A new port in the malpractice storm?
Can hospitals legally subsidize their physicians' malpractice insurance premiums? In a letter posted on the HHS Office of Inspector General's Web site ( www.oig.hhs.gov/fraud/docs/alertsandbulletins/malpracticeprogram.pdf ), Chief Counsel Lewis Morris declines to issue a determination, but suggests that such programs might "fit into employee or physician recruitment safe harbors."
An unnamed hospital chain had sought the OIG's approval of a plan to defray the premium increases physicians face in Florida, Nevada, Texas, and West Virginia. The company's letter spelled out several safeguards: for example, the subsidies would be temporary and not related to the volume of business a physician generates; only active medical staff members would be eligible; and the doctors' share of the payments couldn't be less than they had been paying before the rate increase. Physicians would have to provide services in an amount that equals the assistance they receive.
How doctors and patients rate Rx drug marketing
A substantial number of doctors (41 percent) surveyed by the FDA believes that direct-to-consumer advertising enhances their interactions with patients. The main benefits reported by those doctors? The ads sparked better discussions with patients, and they made patients more aware of available treatments. Few thought the ads educated patients or encouraged patient compliance.
What do patients think about drug companies' advertising to physicians? According to a recent Wall Street Journal Online/Harris Interactive Health-Care Poll, only about a quarter of respondents feel drug marketing to doctors is "acceptable and reasonable," while more than half think it's too aggressive. Still, nearly 7 in 10 trust their doctors to choose the best drugs for them.
This year's Medicare cut turns into a hike
Fearing that continued fee cuts would hinder seniors' access to physicians, the House and Senate enacted legislation enabling CMS to alter the controversial formula used to calculate Medicare's physician reimbursement. After revising the figures used in the statutory formula, CMS increased physician payments by an average of 1.6 percent, instead of cutting them 4.4 percent as originally announced. The new rates will be effective March 1.
Medicine's new malpractice refugees
Many ob/gyns in the 12 states the AMA considers to be in a malpractice crisis are being driven out of practice or, at the very least, forced to change their practice style. So says a recent survey by Merritt, Hawkins & Associates, an Irving, TX-based physician search firm. The surveyed doctors work in Florida, Georgia, Mississippi, Nevada, New Jersey, New York, Ohio, Oregon, Pennsylvania, Texas, Washington, and West Virginia.



The ERISA shield for HMOs shrinks again
Patients in Connecticut, New York, and Vermont will find it easier to sue their HMOs under state medical malpractice doctrines, thanks to a new ruling by the US Court of Appeals for the Second Circuit. The suit, brought by the widow of a man who died after his health plan refused to authorize treatment recommended by his physician, had been dismissed by a lower court on the grounds that all of the malpractice claims "involve eligibility for coverage" and thus were pre-empted by the Employee Retirement Income Security Act of 1974.
While agreeing that claims directly involved with the health plan's administration are protected under ERISA, the appellate court noted that the US Supreme Court had established a new framework for claims where the line between administrative decisions and medical judgment is less clear. In light of the Supreme Court's decision, the appeals court concluded that HMOs may be held accountable under state medical malpractice claims.
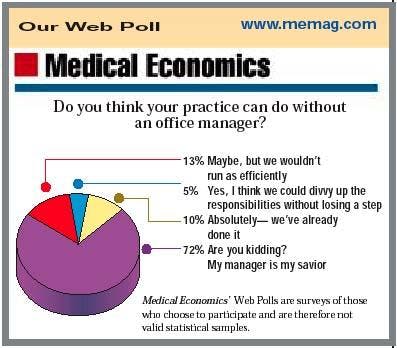
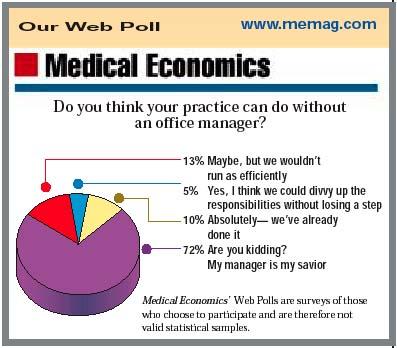
Our Web Poll

SPECIAL REPORT: The Feds issue final HIPAA security rules
The Department of Health and Human Services last month issued a final version of its proposed security standards under the Health Insurance Portability and Accountability Act (HIPAA). Although most of the new rules, intended to secure privacy of electronic patient information, won't take effect until April 2005, you'll be expected to take some steps before that. HIPAA regs are often complicated, and the latest pronouncement is no exception.
Fortunately, there's real flexibility built into the system. HHS notes that this final version focuses more on what needs to be accomplishedsetting up a system to prevent unauthorized people from seeing private patient recordsand less on a specific checklist of exactly how it should be done.
At the most general level, physicians are called on to keep protected information about patients confidential, to guard it "against any reasonably anticipated threats or hazards," to prevent its misuse, and to ensure compliance by adequately training all staff members. Within this broad set of marching orders, physicians have fairly wide latitude, depending on practice size, complexity, and potential risk.
For example, the set of rules dealing with "administrative safeguards" requires that doctors "implement procedures to determine that the access of a workforce member to electronic protected health information is appropriate." The government doesn't tell you exactly what to do. How you achieve that result is up to the doctor, as long as the procedure adopted is reasonable and appropriate to the circumstances. Doctors also get to decide how access to protected data is terminated, if, for instance, a staff member quits or is let go.
In other areas, doctors will have fewer options, especially once the security rules themselves kick in two years from now. For example, there must be "physical safeguards for all work stations that access" electronic health information in order "to restrict access to authorized users." Similarly, in implementing one of a series of technical safeguards, doctors must "assign a unique name and/or number for identifying and tracking user identity."
Not only must doctors follow these rulesbut so must their business associates such as clearinghouses and billing companies. Mere good faith efforts at compliance won't be enough to protect physicians from regulatory enforcement. What will count the most are results, and those "are likely to be judged retroactively," say attorneys at the firm of Davis Wright Tremaine. For this reason, full documentation of the procedures you've implementedand their effectivenesswill be crucial.
To view the new security rules in their entirety, visit the Web site for the Centers for Medicare & Medicaid Services (www.cms.gov ). Click on HIPAA in the left-hand column, and then click on HIPAA Administrative Simplification. For additional information on how to safeguard your computer system, see "The key to a HIPAA-safe computer system" in our next issue.
Wayne J. Guglielmo, Senior Editor
Check with Online Updates
for more news
Joan Rose. UPDATE: Focus on practice. Medical Economics 2003;6:14.











