



Article
Practice Beat
Author(s):
Fraud and abuse; Tommorrow's doctors; Organ transplants; Health insurance; etc......
Practice Beat
By Joan R. Rose, Senior Editor

Fraud And Abuse : Government agencies have a new weapon in their arsenal
Now the federal government has launched the Healthcare Integrity andProtection Data Bank (HIPDB), which will contain information on health care-relatedcivil judgments (excluding malpractice) against a provider or supplier,criminal convictions, adverse licensing and certification actions, and exclusionsfrom participation in federal or state programs. Government agencies andprivate health plans are required to report all such actions taken sinceAug. 21, 1996.
Information reported to the data bank is confidential, and may be requestedonly for use in privileging and employment, professional review, licensing,certification or registration, fraud and abuse investigations, certificationto participate in a government program, and civil and administrative sanctions.Access to HIPDB reports will be limited to self-queries by subjects of thosereports, and to federal and state agencies and reporting health plans. It'sestimated that the HIPDB will process more than 1 million requests for informationduring its first year.
The HIPDB will complement the 10-year-old National Practitioner DataBank. Its day-to-day operations will be managed for the Office of InspectorGeneral by HHS' Health Resources and Services Administration, which alsooversees the NPDB.
Organ Transplants: Uncle Sam: New rules won't make things worse forpatients
In the past, organ allocation policies gave priority to patients basedon their geographic location rather than medical need. Now, under federalrules that went into effect last month, the Organ Procurement and TransplantationNetwork will be required to develop "adequately broad" allocationareas to ensure that organs reach patients who need them most. But the amendedfinal rule doesn't require a "single national list" for allocation,as HHS had proposed earlier.
When HHS first announced its intent to end "local first" policies,critics expressed concern that small transplant centers would be forcedto close, thus depriving patients of local access to donated organs. Butthe perception that patients generally have widespread local access to suchfacilities is a myth, according to an HHS study. In 1997, for example, morethan 80 percent of liver transplants were performed in just 35 cities, and77 of the 117 centers were located in cities with two or more liver transplantcenters. It's the limited number of organs for transplant, not the numberof centers or their location, that imposes constraint on transplants, HHScontends.
A recent report from the Institute of Medicine also noted that therewas no "credible evidence that . . . the new rules would result inthe closure of smaller transplant centers."
Uninsured Children: President Clinton asks doctors to help ease theproblem
The president wants physicians to help meet goals of the Children's HealthInsurance Program.
In a speech before the American Academy of Pediatrics in October, Clintonnoted that when CHIP went into effect in 1997, it was expected to providehealth insurance to some 5 million children. But thus far, just 1 millionyoungsters are enrolled. Only this year, in fact, has every state even gottenits CHIP program in place. Another 2 or 3 million Medicaid-eligible childrenstill aren't covered, the president estimates.
Clinton encouraged the doctors to work with local medical societies,clinics, and schools to make uninsured familiesespecially those whosefirst language isn't Englishaware that they may be eligible for government-fundedinsurance.
Docket Watch: One Pennsylvania doctor cracks the peer review shield. . .
The Pennsylvania Supreme Court has sided with a physician who soughtto obtain an audiotape of an internal hospital proceeding. The doctor hadchallenged the fairness and integrity of a hospital medical board that hadaltered a recommendation made about him by a peer review panel.
The physician's clinical privileges had been suspended in 1995 for "aserious issue involving patient care" that resulted in a medical malpracticesuit. But two years later, a peer review panel unanimously recommended tothe hospital medical board that the suspension be terminated because "thefacts do not support suspension." Before sending that recommendationto the hospital's board of directors, however, the medical board changedthe statement to read "the facts do not support continued suspension."
After a confidential source allegedly told the doctor that some membersof the board had had an ulterior motive in changing the gist of the recommendation,the physician went to court to get an audiotape of the board meeting. Butthe hospital refused to hand it over as ordered by the trial court and filedan appeal. The hospital's board of directors, meanwhile, reinstated thedoctor's privileges, causing the appellate court to declare the appeal moot.
The state Supreme Court found that the lower court had erred. While statelaw affords limited immunity from civil and criminal liability to participantsin the peer review process, the court said, that immunity isn't meant toapply if an individual is motivated by malice. And since the doctor wantedthe tape to learn whether the process had been misused, state law doesn'tbar him from obtaining a copy.
Moreover, the court noted, the revised recommendationbecause itimplied that the original suspension was warrantedwas likely to "continueto have a deleterious effect on the doctor's career if left unchallenged."
. . . while another carves out a broader meaning of informed consent
A surgeon who thought his malpractice woes were behind him will haveto mount a new defense, a Pennsylvania appellate court has ruled.
The case concerns a woman who had undergone surgery for esophageal cancer.She later suffered a rupture of the surgical site, necessitating emergencysurgery and leaving her with permanent lung damage. In the malpractice casethat followed, the woman charged the doctor who had performed the originalsurgery with failure to obtain her informed consent. A jury ruled in thedoctor's favor.
The appellate court's decision to vacate the jury verdict turned on thetrial court's refusal to permit the patient and her husband to offer evidencethat the surgeon had lied about his experience with the procedure. Suchinformation, the trial court had said, had no bearing on the doctrine ofinformed consent.
But the appellate court found that evidence of the doctor's lack of experiencewas relevant. An agreement between a physician and patient is contractualin nature, the judges ruled, and for consent to be valid, both parties mustunderstand the nature of the undertaking and the possibleas well asthe expectedresults. Since a reasonable person would consider suchinformation significant, a physician who provides false information whenquestioned would be subject to a claim of lack of informed consent.
Physician Recruitment: Specialists find the warmest welcome in years
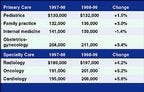
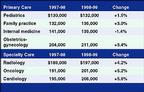
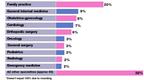
Specialists have replaced primary care physicians as the doctors mostwanted by hospitals, group practices, and other health care organizations,according to Texas-based Merritt, Hawkins Associates, a national physicianrecruiter. Indeed, an analysis of 1,807 searches the firm conducted fromApril 1998 through March 1999 found that demand for specialists has madean enormous comeback. In 1995-96, 72 percent of MHA's searches focused onprimary care physicians. In 1998-99, 61 percent involved specialists.
Average salaries offered to the most in-demand physicians

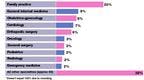
(% of all searches*)
Doctors on recruiters' most-wanted list

Types of incentives/perks offered



(% of potential employers offering each)
Looking Ahead
A handy reference of telephone numbers, as well as e-mail and Web siteaddresses for some sponsoring organizations.
January
131 Birth Defects Prevention Month
March of Dimes Birth Defects Foundation
1275 Mamaroneck Ave.
White Plains, NY 10605
Phone: 888-MODIMES
Fax: 914-997-4763
E-mail: resourcecenter@modimes.org
Web site: www.modimes.org
131 National Eye Care Month
American Academy of Ophthalmology
655 Beech St.
San Francisco, CA 94109-1336
Phone: 415-561-8500
Fax: 415-561-8533
E-Mail: nanderson@aao.org
Web site: www.eyenet.org
131 National Glaucoma Awareness Month
Prevent Blindness America
500 East Remington Road
Schaumburg, IL 60173
Phone: 800-331-2020
Fax: 847-843-8458
E-mail: info@preventblindness.org
Web site: www.preventblindness.org
131 National Thyroid Awareness Month
American Association of Clinical Endocrinologists
PO Box 3426
Grand Central Station
New York, NY 10163
Web site: www.aace.com
1-31 National Volunteer Blood Donor Month
American Association of Blood Banks
8101 Glenbrook Road
Bethesda, MD 20814-2749
Phone: 301-907-6977
Fax: 301-907-6895
E-mail: christine@aabb.org
Web site: www.aabb.org
Joan Rose. Practice Beat. Medical Economics 1999;23:30.










