Article
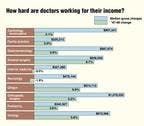
How much are groups paying their doctors?
With more practices tying compensation to productivity for all doctors, primary care can kiss its subsidy goodbye.
Group Practice Economics
How much are groups paying their doctors?
With more practices tying compensation to productivityfor all doctors, primary care can kiss its subsidy goodbye.
By Anita J. Slomski, Group Practice Editor

Talk to any physician recruiter, and you'll hear that 1999 has been theYear of the Specialistand the trend shows every sign of continuing."If you're a cardiologist, dermatologist, urologist, or pulmonologist,life is grand," declares Mark E. Smith of the recruitment firm of Merritt,Hawkins and Associates. "Just tell us where you want to live and we'llfind you a position." Even the beleaguered anesthesiologists, recentlythe butt of doctor-unemployment jokes, are considered a hot search to- day."A few years ago, I steered medical students away from anesthesiology,"recalls Smith. "The advice was accurate at the time, but it's deadwrong now."
For the first time in the six years that Merritt, Hawkins has compiledits recruitment survey, specialist searches have outnumbered those for primarycare doctors. In the fiscal year ended March 31, 1999, 69 percent of thesearches were for specialistscompared with 72 percent for primarycare physicians in l995-96. "This is the most radical and rapid shiftin the demand for specialists I've seen in 10 years," Smith says.
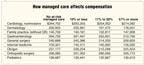
Specialists also outpaced primary care doctors in pay hikes during thecalendar year 1998, according to the Medical Group Management Association'sannual survey of 1,609 group practices. Median compensation for specialistsincreased 5.2 percent, while median primary care salaries went up only 2.5percent. During the previous year1997compensation for both specialistsand primary physicians was basically flat. The American Medical Group Association,which exclusively surveys large multispecialty groups, also reported biggergains for specialists: a 1.25 percent increase vs a 2.4 percent decreasefor generalists in 1998.
What's going on here?
Technology boosts specialists' pay
The recruitment frenzy for specialists is simply a matter of supply anddemand. During the 1990s, medical students were often advised to enter primarycare because of the perceived glut of specialists. But just as the flowof young specialists began to ebb, aging baby boomers began needing specialtyservices in large numbers. At the same time, many managed care plans wereeasing up on their use of gatekeepers, allowing patients direct access tospecialists. And patients began making appointments.
The shift in demand led to a change in the way groups approach compensation.After several years of giving primary care doctors bigger salaries thantheir production supported, some larger multispecialty groups tweaked compensationformulas to reduce the primary care subsidy and transfer more revenue tospecialists. "These groups are afraid they'll lose specialists whoare vital to their survival, or they won't be able to hire the specialiststhey need if they don't pay them more," says Shawn D. Schwartz, managerwith the national health care consulting division of RSM McGladrey, whichcompiles AMGA's compensation survey.
Some lucky specialists are making more money because patients are willingto pay out-of-pocket for their services. Ophthalmologists are benefitingfrom the interest in lasik surgery, for example, while dermatologists andplastic surgeons are cashing in on baby boomers' yen for everlasting youth."A few years ago, a group could hire a plastic surgeon for a song,but that's no longer true," says Michael Parshall, a consultant withThe Health Care Group in Plymouth Meeting, PA. "There's interest incatering to patients now, and groups are hiring doctors to do that. Forinstance, I have an FP client who went to China to learn about mixing theherbs his patients want."
Although a 5 percent increase in compensation is no windfall, it's morethan many specialists had hoped for, given earlier predictions about a hostilepayer climate. "The conversion to the RVU payment scale was supposedto gut specialists' fees, but it didn't cause as much damage as expected,"says Steve Rice, vice president of MSA Physician Services, a health careconsulting subsidiary of MMI Companies, based in Kansas City, MO. "Andcapitation didn't take hold like people predicted, so specialists are stillbeing paid discounted fee-for-service, which is maintaining their incomes.With the gatekeeper out of the way, we're seeing specialists get much moreaggressive about seeking associations with IPAs or primary care networksto protect their patient base."
Likewise, specialists' incomes are rising in groups that "right-sized"in anticipation of managed care. In those groups, where the ratio of primariesto specialists is greater, the specialists are kept extremely busy.
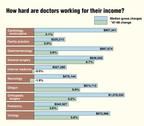
And therein lies the rub. Although primary care physicians and specialistshave had almost identical pay raises in the last five years9.1 and9.3 percent, respectivelyspecialists have had to work much harderfor theirs. According to MGMA data, production among primary care doctors(as measured by median gross charges) rose 11.6 percent during that half-decade,while specialists ramped up their production by 29.3 percent.
Today, with the shift in demand and groups' willingness to pay specialistsaccordingly, the wind has shifted. "There is no national shortage ofgeneralists nowjust regional allocation problems," says DavidGans, survey operations director for MGMA. "So groups have begun payingprimary doctors salaries based more on their actual production." Andfor primary doctors, that is the rub.
Seeing more patients would increase their pay, of course, but some arealready seeing as many as they possibly canand their income potentialhas maxed out. Specialists, on the other handalready paid by straightproductioncan take advantage of new technology to do more procedures.For those who've long harbored grudges against primary doctors for "coasting,"these are satisfying days.
There is a hint of a silver lining for primary care doctors, however."Primary physicians will see a slow but steady increase in their salariesbecause payers are still placing a premium on diagnostic, rather than procedural,skills," says Gans. And specialists will see their salaries decreaseas they reach their workweek limit. "Many specialists alreadywork 55-hour weeks," says Gans. "And one thing is for sure: Paymentfor those hours is not going to go up. Expenses will continue to increasewhile reimbursement to specialists will remain constantor actuallydecrease due to managed care pressures."
That long-term outlook is not good news for any physician, or for thoseconsidering medicine as a career. In 1999, medical school applications fellfor the third straight yearthe result, some say, of flat incomes."Physicians will always be paid a good salary," says Gans. "Butif you want a high salary, be a stockbroker or computer scientist.People will have to go into medicine for other reasons."
Enterprising doctors find other ways to boost income
Short of working around the clock, what can you do to increase productivity?Many groups are now hiring midlevel providers, which can add $20,000 to$80,000 a year to physicians' income, according to consultants. "Veryefficient primary care doctors give well- or routine-care patients to aPA or nurse practitioner," explains C.J. Bolster, managing directorfor the Hay Group. "That way, they function more like specialists andplay the volume gameseeing as many sick patients as they can."
Ironically, specialists, in order to increase their compensation, areemulating generalists by taking on more management of chronic disease. Anoncologist, for example, may treat a cancer patient's cold or flu becauseof complicating factors with the patient's immune system. "He getsto bill for more patient encounters, and that kind of comprehensive careis better for the patient," says Bolster.
Gainsharing, which rewarded doctors for participating in hospitals' qualityimprovement and cost-containment programs, was killed this year when theOffice of Inspector General declared these arrangements illegal. "Thereare some ways to work around the ruling," says James Rodegehero, directorof physician compensation for Ernst & Young. One possibility is to partnerwith hospitals to improve clinical outcomes and protocols. Rodegehero acknowledges,however, that the dollar amount won't be as significant as doctors mightlike.
In an effort to increase revenue, groups are also hiring more full-timemedical directors and physician administrators so that the rank and filespend less time in committee meetings and more time seeing patients. Butthose directors, charged with monitoring doctors' utilization and practices,are moving groups back toward 100 percent production-based compensationwithits built-in limits on primary physicians' incomes.
"Compensation formulas are becoming simpler because the complicatedones didn't send doctors the right messageto work harder," saysRodegehero. "So the pendulum is swinging back to basing pay on classicgross charges or RVUs, which is counter to what managed care tells us todo. Groups are reverting to a model they know works, and letting medicaldirectors manage the side effects of utilization."
Given all that, who exactly is hot?
Working doctors may bemoan their long-term compensation potential, butnew recruits couldn't be happier about the offers coming their way. RecruiterMark Smith's hottest search is for cardiologists, driven by cardiology PPMsaggressively expanding their practices and baby boomers experiencing thefirst signs of heart disease. And with better technology and drugs, there'sless need to refer to cardiovascular surgeons. "Offers to cardiologistshave increased by $50,000 to $100,000 in the last 18 months," saysan incredulous Smith.
Groups are luring dermatologists with pay packages that are $30,000 to$50,000 higher than they were a year ago, according to Smith. "Dermatologistshave a very lucrative cash business on top of their traditional practice.They can do hair removal and peelings, and they're seeing a high volumeof skin cancer on people who worshiped the sun before we knew better."Other doctors easy to place these days include oncologists, urologists,gastroenterologists, pulmonologists, orthopedists, and the new specialtyof interventional radiologist.
Competition is also driving the recruiting demand. "If one groupexpands, two others in the area may feel they have to do the same,"says Smith. "So you'll have three groups recruiting the same specialistto take care of the same 25,000 people." And in the rush to capturepatients, groups in outlying communities are adding specialists, too. Aftera visiting cardiologist from the big city builds up a patient base in acountry hamlet, for example, the rural group will likely want to keep thoserevenues for itself by hiring its own cardiologist.
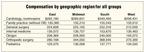
Not surprisingly, physicians continue to earn more in rural and lesscosmopolitan areas. One Mayo-trained plastic surgeon was offered $100,000in Minneapolis, which he turned down for $250,000 in Omaha, says consultantSteve Rice. Primary doctors are commanding $150,000 or more, plus a signingbonus, to practice in the country.
Although more physicians are interested in part-time or flexible schedules,Rice cringes whenever he hears young physicians say they want to "havea life." One new primary doctor in Colorado told Rice he preferredto work only four days a week so he would have time to "walk in thewoods and sniff the pinecones." That's great, says Rice, "buthe still wanted reduced hours and $130,000 with a bonus based not on productivitybut on patient satisfaction or access."
Besides dealing with unrealistic expectations from doctors, groups continueto struggle over how to accommodate physicians who want to work half-time.One big problem is that rich benefits packages aren't easy to divide. "Thereis no way that a physician working half-time offsets the cost of the benefits,"says Rodegehero. Another issue is that part-timers tend to be less productive,although women often put in extra effort to see their share of patients,says Rice. "Part-time female ob/gyns are like gold; they put in almostas many hours as a full-time doctor," Rice observes."
One final note to physicians who study compensation data: If there isa minus sign in front of your specialty's change in compensation, take heart.Next year it may be a plus. "Physician compensation is cyclical innature," says Schwartz of RSM McGladrey. "Look for five- or seven-yeartrends; they may account for the up and down cycles. Just be sure you'rein a reasonable range."
MGMA's Gans is "optimistic" about compensation in the shortrunthat is, the next three years. But he predicts most physiciansprimariesand specialistswill have reached maximum production by 2003. And thenthings will really get flator worse. Nobody will be able to work moreto earn more.
So look at it this way: For now, you have a three-year reprieve.

















Anita Slomski. How much are groups paying their doctors?. Medical Economics 2000;1:115.